Adenomyosis affects the muscle wall of the uterus.
The endometrium is the lining of the uterus (womb). Adenomyosis is when tissue, similar to this lining, grows in the muscle wall of the uterus. During your period, this tissue can thicken, break down and bleed, causing painful and heavy periods.
Adenomyosis can also cause the uterus to enlarge and put pressure on your lower abdomen.
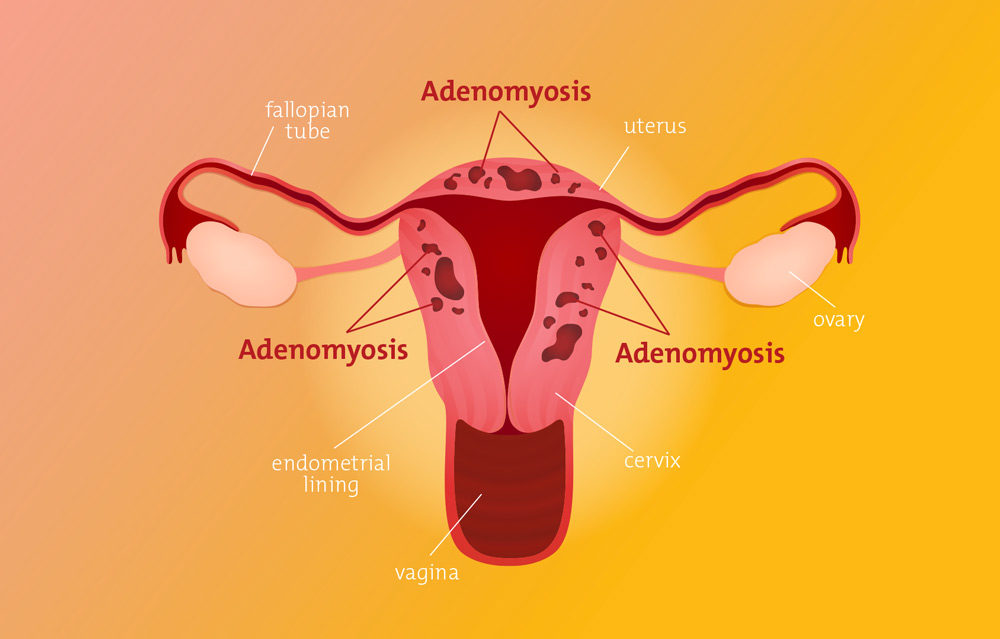 Diagram of uterus with adenomyosis
Diagram of uterus with adenomyosis Symptoms
Symptoms of adenomyosis can include:
- period pain
- pelvic pain
- pain before and after your period
- abnormal, heavy or prolonged menstrual bleeding
- infertility
- painful sex.
Causes and risk factors
About 20 to 35 per cent of women have adenomyosis (source: RANZCOG Endometriosis Clinical Practice Guideline).
The cause of adenomyosis is still unknown .
Many people with adenomyosis also have endometriosis, and vice versa.
Adenomyosis becomes more common with age, and more common after carrying pregnancies.
Diagnosis
A pelvic exam, ultrasound and/or MRI help your doctor investigate whether adenomyosis is the cause of your symptoms. This allows for a clinical diagnosis of adenomyosis, which is based on a combination of symptoms and imaging.
Adenomyosis can be suspected on hysteroscopy or laparoscopy surgeries.
The most accurate way to diagnose adenomyosis is in the lab, by examining tissue excised (surgically removed) from the uterus. This can only be done at the time of hysterectomy, so your doctor most often relies on clinical diagnosis.
Pelvic exam
With your consent, and if appropriate, your doctor can perform a pelvic exam to check if the uterus is enlarged or tender. This examination involves the doctor using their hand to feel the uterus and its supporting ligaments through the vagina.
Ultrasound
An ultrasound creates an image of internal organs using sound waves. A high-quality pelvic ultrasound can see moderate to severe adenomyosis and lead to a clinical diagnosis. A transvaginal ultrasound will show more detail than a transabdominal one.
MRI scan
In some cases, an MRI is suitable to investigate adenomyosis and lead to a clinical diagnosis. The MRI machine creates detailed, cross-sectional images of your organs and tissues.
Laparoscopy
Often signs of adenomyosis may be seen on laparoscopy. Laparoscopy is a keyhole surgery, used for the visual diagnosis and treatment of endometriosis and investigation of other causes of pelvic pain.
Pathology test of the uterus
The conclusive way to diagnose adenomyosis is for a pathologist to examine tissue from the uterus under the microscope. This is only possible with a hysterectomy: surgery to remove the uterus. This is not suitable for everyone because it is an irreversible procedure and means you cannot carry a child afterwards.
Treatment and management
Treatment for adenomyosis is personalised depending on your symptoms, severity and plans for pregnancy.
Hormone therapy
Because adenomyosis is mostly oestrogen-dependent, hormone treatment can help reduce heavy menstrual bleeding and painful periods. Adenomyosis responds to the same hormones as endometriosis which is useful when they occur together.
Common types of hormone therapy:
- progestogens – such as a progestogen-releasing intra-uterine device (IUD) or oral, implanted or injected progestogens. The IUD is particularly effective as the hormone is absorbed directly into the affected muscle.
- combined oral contraceptive (birth control) pill.
Other types of hormone therapy for adenomyosis:
- gonadotropin-releasing hormone (GnRH) analogues
- aromatase inhibitors.
Hormone therapy is suitable for people wanting to be pregnant in the future, as you can remove or stop taking it.
Hysterectomy – removal of the uterus
Hysterectomy is a known cure for adenomyosis, and the condition will not return afterwards. A specialist gynaecologist performs this surgery to remove the uterus, fallopian tubes, and usually the cervix.
It is not suitable for people planning pregnancy in the future. A hysterectomy is irreversible and means you won’t be able to carry children.
Pain management
Non-pharmacological (not involving medication)
Heat including baths and heat packs offer relief from pain secondary to adenomyosis.
Exercise has been proven to reduce pain for many pain conditions by the release of endorphins. Avoid exercises that worsen pain, which may be things like running, and use other types such as swimming or cycling.
Pharmacological (medication)
Analgesics (also known as pain killers) are medications that can help relieve your pain:
- Non-steroidal anti-inflammatory drugs (NSAIDs) such as Ibuprofen and Naproxen.
- Paracetamol can relieve pain and prevent pain worsening when taken early, especially when combined with NSAIDs.
- Opioids – opioids are strong, addictive medication which have no role in the long term management of pain. While they can be effective, risks and harms outweigh benefits over the long term.
Read a digital copy of our Endometriosis Pain Management Guide to learn more about pain and strategies to manage it. While written for endometriosis, the strategies are relevant to adenomyosis too.
Other treatments:
-
Endometrial ablation
Endometrial ablation involves burning the lining of the uterus. It is performed under general anaesthetic. It can assist with heavy bleeding secondary to adenomyosis (and other conditions), but rarely improves pain and has the potential to worsen pain depending on the severity of the adenomyosis.
You are no longer able to conceive after endometrial ablation, so it is only used if you do not plan to conceive a pregnancy in the future.
-
Uterine artery embolisation
Uterine artery embolisation is a procedure where the blood supply to the uterus is intentionally interrupted to cause the uterus to shrink. It rarely has a role in the management of adenomyosis.
-
Adenomyomectomy
Occasionally, adenomyosis can be contained in one area or lump, known as an adenomyoma. There are some circumstances where removing just that part of the uterus is the best course of action.
-
Complementary therapies
Complementary therapies, including acupuncture and CBD oil have been useful for some patients, however evidence is lacking at this point in time.
Some people find complementary therapies useful to manage pain and symptoms of adenomyosis. You may like to trial these and find what works for you, for example:
- guided image therapy
- hypnotherapy
- massage
- meditation
- music therapy
- naturopathy
- yoga.
Adenomyosis specialists
A gynaecologist is a doctor specialising in the diagnosis, medical treatment and surgical treatment of gynaecological conditions. Not every gynaecologist has experience in adenomyosis, so finding a specialist that suits your needs is important.
For help finding a specialist for adenomyosis and/or endometriosis in Victoria, you can browse our specialists or contact our nurse coordinator at the Julia Argyrou Endometriosis Centre at Epworth. They can schedule a nursing review, introduce Epworth specialists and write a recommendation letter to your GP.
Fertility and pregnancy
Adenomyosis is common. Many patients with adenomyosis achieve successful pregnancies despite this – and sometimes without even knowing they have it. There is also an increased risk of early pregnancy loss with adenomyosis.
The severity of adenomyosis is calculated based on the volume of the uterus. For many people with adenomyosis there is minimal increase in uterine volume, meaning a lower risk of fertility complications.
If you are concerned about adenomyosis and fertility, you should speak to your specialist about how it is likely to affect you.