
Dr Kate Tyson is a gynaecologist, advanced laparoscopic surgeon, and the inaugural Director of the Julia Argyrou Endometriosis Centre at Epworth. Dr Tyson answers common questions about laparoscopy – part of the surgical diagnosis and treatment of endometriosis.
What is a laparoscopy?
Laparoscopy is a type of minimally invasive surgery. It is used to diagnose and treat endometriosis (as well as other diseases). It involves small incisions on the abdominal wall, using gas to distend the abdomen and allow visualisation of the structures inside. Even very complex surgery can be undertaken by laparoscopy, including treatment of endometriosis and investigation of infertility.
What happens during the surgery? What are the risks?
Your surgeon will perform the laparoscopy while you are under general anaesthetic. Usually there will be two to four 0.5-1cm incisions on the abdomen where ports have been used to pass instruments inside to treat endometriosis.
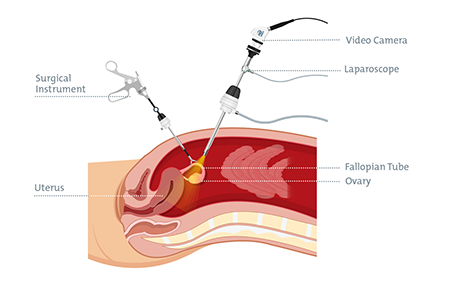
Diagram: Instruments and location of a laparoscopy for endometriosis
To diagnose endometriosis, your surgeon examines the inside of the pelvic and abdominal cavities and removes samples of tissue if they look suspicious for endometriosis. A pathologist then examines these tissues under the microscope to confirm if endometriosis is present.
During laparoscopy, your surgeon will remove or destroy any visible endometriosis (endometrial implants). They will discuss the method they plan to use at the time of consultation:
- Ablation, fulguration or vaporisation – to destroy endometrial implants.
- Excision – to cut out implants.
Laparoscopy is considered generally safe, although risks include damaging other structures inside the tummy, like the bladder or bowel, or needing to convert to open surgery in a small percentage of cases.
The most common side effect is pain from gas trapped under the diaphragm. This usually passes after the first 48 hours. Occasionally, disease may be more severe than expected, and your surgery may need to be completed on another day or with another surgeon, such as a colorectal surgeon.
What is the laparoscopy recovery time for endometriosis?
Each patient is different and the amount of time they need to take off work will vary. Also, the small size of the incisions on the abdomen don’t reflect what may have been quite extensive surgery inside.
For many patients, two weeks off work or school is enough, although some mild discomfort and fatigue may persist a little longer.
Recovery from more major surgery may take longer. Smaller holes in the abdomen generally means less pain, and a quicker return to normal function.
Who performs a laparoscopy for endometriosis?
Laparoscopy for endometriosis is best performed by specialist gynaecologists who diagnose and treat endometriosis regularly.
Some types of endometriosis, including stage 4 endometriosis or endometriosis involving the bladder or bowel, require your gynaecologist to have advanced surgical training to be able to safely perform the surgery. An example of this training is A.G.E.S. training.
To ensure your gynaecologist is the right fit for you, you can ask about their experience in treating endometriosis or their surgical experience and training. Our Nurse Coordinator at the Julia Argyrou Endometriosis Centre at Epworth can help you find an Epworth specialist with extensive experience treating endometriosis.
Is there other surgery that may be part of endometriosis treatment?
A hysteroscopy (passing a camera into the uterus from the vagina) is often performed at the same time as a laparoscopy, to ensure the cavity of the uterus is normal. Your gynaecologist may also recommend an IUD as treatment for endometriosis, which can be inserted during the laparoscopy.
A hysterectomy (removal of the uterus) may be recommended for some patients, which can be beneficial when adenomyosis is also present and is not responding to medical treatment.
In a small number of patients, endometriosis may invade other nearby organs, including the bladder and bowel. If this occurs, your gynaecologist may recommend surgery with another specialist surgeon e.g. urologist or colorectal surgeon.
What should someone consider when making decisions about surgery?
Your gynaecologist will give you the information you need to inform a decision about surgery for endometriosis. Some surgery can affect fertility and may worsen pain. Having as few surgeries as possible limits these complications.
While it is difficult to generalise about endometriosis, medical treatment should be used as the first line treatment with surgery reserved for specific situations.
Is there research on non-surgical ways to diagnose endometriosis?
There is a lot of work happening in the research space to find other non-invasive ways to diagnose endometriosis, including using blood tests or even menstrual fluid. Clinical algorithms also allow for better prediction of patients likely or less likely to have endometriosis.
The Julia Argyrou Endometriosis Centre at Epworth can support you to access specialist and allied health care at Epworth, tailored to your needs. Contact our dedicated Endometriosis Nurse Coordinator with any questions or to schedule a nursing review.
31 August 2022